
In the intricate world of medical device commercialization, one of the pivotal factors determining market success is the ability to secure reimbursement. Companies invest years and millions of dollars in designing their product, obtaining its regulatory clearance/approval, developing appropriate clinical data, and making decisions regarding its price, but they often do so without considering who would eventually need to decide whether or not to pay for their product.
The entity which will make this decision might be a payer (sickness fund/health insurer), a hospital, a physician group, or an accountable/integrated care organization (to name a few examples). When considering its reimbursement/funding decision, each of these entities may assign different values to different product features, a different “intended use” in the regulatory clearance/approval document, different clinical data points, and a different price structure. Working on a medical product without first identifying who your reimbursement decision maker is, is like preparing for the World Steak competition in order to offer a costly steak to a penniless vegetarian, or hiring a vegan chef to recommend a quinoa salad to a dedicated carnivore.
In this focused exploration, we delve into the critical role of identifying the relevant decision maker in order to facilitate the development of the right product, the appropriate wording on the product’s regulatory clearance/approval document, the required clinical data points, and the most relevant pricing structure—all designed to meet the needs of the identified reimbursement decision maker. Partnering with a specialized medical device reimbursement consulting firm early in development ensures a robust medical device reimbursement strategy is mapped before freezing your clinical trials.
Reimbursement Model 1: Payers as the Medical Device Reimbursement Decision Makers
Under traditional Fee-for-Service reimbursement systems, when a patient needed surgery (e.g., knee replacement), the payer paid for each provided service – a service-centric reimbursement system. Thus, the payer paid the imaging facility for the CT scan, paid the physician for determining the patient’s diagnosis, planning the surgical procedure and performing it, paid the hospital for its associated services in facilitating the surgical procedure, paid the anesthesiologist and paid the physical therapist for the patient’s rehabilitation process post-surgery.
In order to pay for each of these separate services, the payer needed a way to separately indicate each service, and this was typically done with a dedicated code. This situation meant that if your company planned to develop a new imaging modality, a new physician diagnostic tool, a new wound dressing or a new rehab device, a new code had to be developed. In addition, the payer had to make a decision about the coverage of this new code; would it be paid for by the payer or not, making the payer the ultimate decision maker for the reimbursement of each and every medical service.
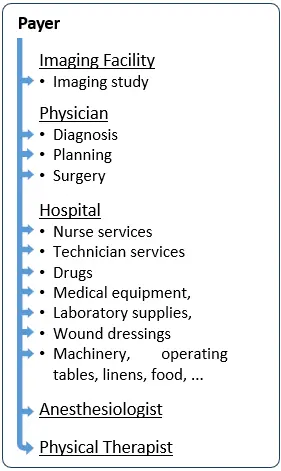
In the chart on the right, each of the little blue arrows indicates a separate service and a potential separate code, requiring a separate coverage decision by a payer.
Reimbursement Model 2: Hospitals as Medical Device Reimbursement Decision Makers
The need to specifically approve each and every discrete medical service by the payer became cumbersome and led to inefficiencies. This started to change in the 1980s, with the introduction of Diagnosis-Related Groups (DRGs), first in the US and subsequently in Europe. DRGs changed the way hospitals are reimbursed and moved from a service-centric reimbursement system to a provider-centric reimbursement system.
Under the DRG method, each hospitalized patient is assigned to a single DRG, under which cases with similar clinical conditions and resource utilization patterns are grouped (e.g., total knee replacement). Each DRG is assigned with a pre-determined, single payment rate, that is paid to the hospital regardless of the actual number of discrete medical services provided to the individual patient by the hospital. It does not matter how many lab tests, wound dressings, drugs or nurses are assigned by the hospital for the treatment of a specific patient. The hospital receives the same pre-determined single lump-sum for every patient undergoing total knee replacement. The hospital also decides how to allocate this single lump-sum to finance required lab tests, medical devices, drugs and nurse time.
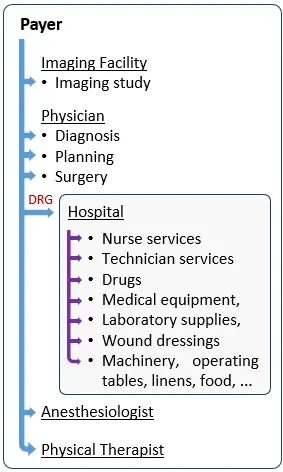
This not only shifts the financial risk associated with the treatment of a patient under a specific DRG from the payer to the hospital, but also turns the hospital into your main decision maker, in case your company develops a component that falls under a specific DRG.
As can be seen in the chart on the right, instead of multiple arrows for each discrete component within the hospital, the payer now pays the hospital a single DRG rate and the hospital becomes the decision maker, who decides which devices to purchase, how to use them, and negotiates their prices. In such case, the payer is indifferent to the type, number or price paid by the hospital for your medical device.
Reimbursement Model 3: Accountable and Integrated Care Organizations as Decision Makers
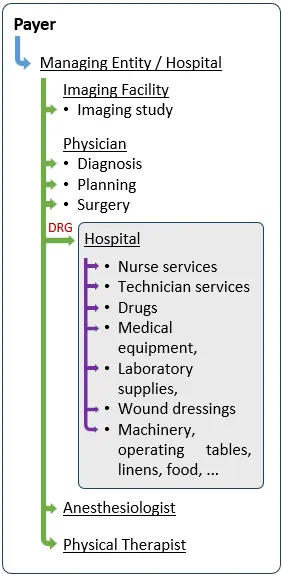
The development of accountable/integrated/bundled care organizations, which is applied in both the US and Europe, signifies a further shift from a provider-centric reimbursement system to a patient-centric one. Instead of paying each provider, the payer contracts with a managing entity (which may also be one of the participating hospitals), to manage the overall care provided by all network providers (imaging centers, physicians, hospitals, rehab facilities) to beneficiaries who voluntarily agree to receive care under this arrangement.
The accountable/integrated/bundled care agreement may cover a specific procedure (e.g., total knee replacement), a specific disease (Diabetes) or all care provided to a participating beneficiary over the course of a certain time period (e.g., a year). The payer typically pays a single lump-sum per participating beneficiary and the managing entity negotiates the allocation of funds with each of the participating providers. In this case, the payer is not involved in the decision-making process concerning utilized medical devices. The managing entity becomes your main decision maker.
As can be seen in the chart on the right, instead of multiple arrows for each provider, the payer now pays the managing entity a single lump-sum per participating beneficiary, and this managing entity becomes the decision maker who decides which devices to purchase for its network providers and negotiates their prices.
Strategic Implications of Choosing the Wrong Reimbursement Decision Maker
As illustrated above, a physician, a hospital, an Accountable or Integrated Care Organization, or a payer may impose very different requirements before agreeing to reimburse a medical device. These requirements may relate to product features, clinical evidence, regulatory approval language, economic value demonstration, or pricing structure.
Developing a product with the wrong reimbursement decision maker in mind can lead to fundamental strategic misalignment. Companies may invest in features that are irrelevant to the actual decision maker, pursue a regulatory strategy that fails to support coverage requirements, or design clinical studies that do not generate the endpoints required for positive reimbursement decisions.
In practice, these missteps often surface late in development — sometimes after regulatory approval — at which point correcting them may require additional studies, labeling changes, price concessions, or even a complete repositioning of the product. These delays increase development costs, extend time to market, and significantly raise the risk of commercial failure.
Clarifying the reimbursement decision maker early is therefore not a tactical detail, but a foundational strategic decision that directly influences product design, regulatory planning, clinical development, and pricing strategy.
A Structured Approach to Identifying the Right Reimbursement Decision Maker
To identify the correct reimbursement decision maker, we recommend starting with a structured assessment early in development to map out your path to global medical device reimbursement. This includes mapping money flows and financial incentives associated with the use of the product, identifying applicable reimbursement mechanisms such as codes, coverage policies, and payment systems, and determining which entity ultimately bears the economic risk.
This analysis enables companies to clearly establish whether reimbursement decisions will be driven primarily by payers, hospitals, physicians, or integrated care organizations, and under which circumstances. Importantly, this step should be completed before finalizing product design, regulatory strategy, clinical study protocols, or pricing assumptions.
By validating these elements early and, where possible, engaging directly with decision makers for feedback, companies significantly reduce reimbursement risk and improve their chances of achieving timely market access and sustainable commercial success.
Key Takeaways
- Identify the correct reimbursement decision maker early.
- Align regulatory, clinical, and pricing strategy to their requirements.
- Understand whether payers, hospitals, or integrated care organizations drive coverage.
Frequently Asked Questions About Medical Device Reimbursement Decision Makers
What is a medical device reimbursement decision maker?
A medical device reimbursement decision maker is the entity that ultimately decides whether a medical device will be paid for and under what conditions. Depending on the reimbursement model, this may be a payer, a hospital, a physician group, or an accountable or integrated care organization.
Why is it important to identify the reimbursement decision maker early?
Identifying the reimbursement decision maker early is critical because it directly influences product design, regulatory strategy, clinical evidence requirements, and pricing. Developing a product without clarity on who will decide reimbursement often leads to misaligned clinical studies, delayed coverage, and increased commercialization risk.
Is the payer always the medical device reimbursement decision maker?
No. While payers often make reimbursement decisions under fee-for-service systems, hospitals are frequently the decision makers under DRG-based payment systems. In integrated or bundled care models, the decision maker may be an accountable or integrated care organization rather than the payer.
How does the reimbursement decision maker affect clinical study design?
The reimbursement decision maker determines which clinical endpoints, comparators, and economic outcomes are required for coverage. For example, payers may focus on population-level outcomes and cost-effectiveness, while hospitals may prioritize operational efficiency and budget impact.
Can choosing the wrong decision maker delay market access?
Yes. If clinical or regulatory strategies are designed around the wrong decision maker, additional studies, labeling changes, or economic analyses may be required after regulatory approval. These delays increase development costs and can significantly postpone reimbursement and market adoption.
How can companies determine the correct reimbursement decision maker?
Companies can determine the correct reimbursement decision maker by mapping reimbursement pathways, understanding applicable payment mechanisms, and analyzing who bears the financial risk associated with product use. Engaging early with payers, hospitals, or integrated care organizations can further validate this assessment.
Need Concrete Market Access Support?
Securing coverage and coding is the most critical step of your commercialization timeline. Our team maps global reimbursement pathways directly to your business goals.
About the Author
