
Dispelling Medical Device Reimbursement Myths
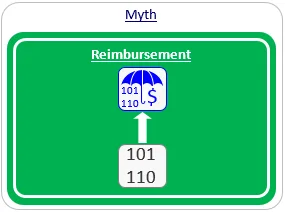
Myth #1: Code = Reimbursement.
One of the first questions we are typically asked when conducting our first meeting with a medical device company's CEO (typically also the entrepreneur) is: "Is there an existing reimbursement code for my device?"
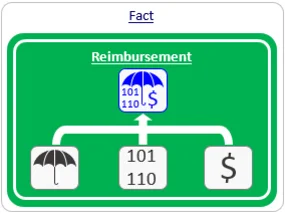
However, reimbursement is comprised of three distinct aspects of the healthcare system:
(1) code, (2) coverage and (3) payment rate.
(depicted in the 'Reimbursement Pillars' diagram).

To many of our clients, a 'code' was initially seen as the only precondition for reimbursement (depicted by the blue symbol on the right). The perceived straight arrow connection between a code and reimbursement is depicted in the 'Myth' image on the right.
But, this is not the case. In order for a device to be reimbursed, the relevant decision-makers (typically health insurance companies or sickness funds, collectively referred to as 'payers') first decide whether the device is 'covered', and if so, how much they will pay for it (i.e., the applicable 'payment rate').
In many cases, the existence of a code is merely a technical convenience used to facilitate smooth communication between healthcare providers (i.e., physicians and hospitals) and payers. In fact, a device may be assigned with a code even though it is not covered, in which case, there is no reimbursement.
Myth #2: There is either full reimbursement or no reimbursement.
When medical device companies embark on the process of obtaining reimbursement for their new device, they typically think of a binary outcome: either their device obtains national reimbursement or it does not. This notion is depicted in the 'Myth' image on the right.
However, devices seldom move from 'no reimbursement' straight to 'national reimbursement'. More often, the company may first be reimbursed using grants that enable hospitals to spend money on certain technologies or for certain patients. Similarly, certain charity funds may allocate some of their budgets to finance specific medical devices or technologies for the benefit of their members. Although such funding resources may require more documentation and manual labor (calling the fund, sending letters, appealing decisions, etc.), it might be the only way for a company to establish its first commercial user base and gather the required evidence, before moving on to the next stage.
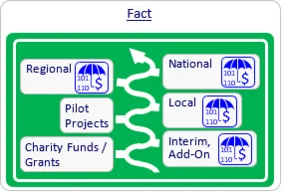
Once it has established an initial user base and real-life evidence, the company may next seek interim, add-on reimbursement by utilizing specific mechanisms in each country (e.g., Innovation Fund or the NUB mechanism in Germany, LPPR add-on List in France or New Technology add-on payments in the US).
At the same time, the company may approach local payers in an attempt to collaborate by conducting a pilot project, which tests the utilization of the new device for a limited time period. At the end of this period, conclusions regarding the reimbursement of the device on a local, regional or national level may be made.
Myth #3: Reimbursement decision-makers in each country use different criteria.
We are often asked by potential clients where they should first launch their product. In order to answer such a strategic question, one has to carefully analyze the different potential markets, map the reimbursement and regulatory landscape in each potential market, identify potential distributors and verify the support of the local medical community - all in relation to the specific product in question.
Many people are under the impression that each country employs different criteria when considering which products will be reimbursed. This assumption is depicted in the 'Myth' image on the right.
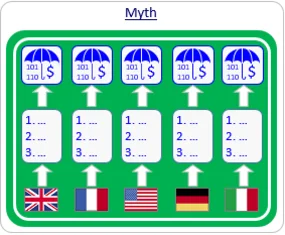
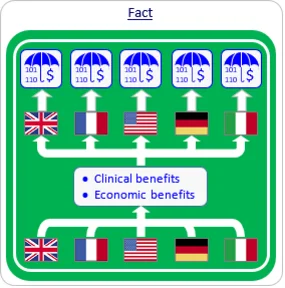
This myth may be correct in some esoteric cases, but in 99% of the cases, reimbursement decision-makers in all countries would consider the following two criteria:
- Will the use of the new medical device provide significant clinical benefits compared with the best utilized alternatives?
- Will the use of the new device provide economic benefits compared with the current medical pathway?
Therefore, if we are able to generate evidence demonstrating compliance with the above two criteria, your device will be reimbursed in all countries. The challenge is to develop the right clinical and economic claims and substantiate them with evidence.
Pro Tip: The Budget Impact Model
Substantiating "economic benefits" usually requires a formal Budget Impact Model (BIM). This tool shows a payer exactly how adopting your device will change their total spend over 1–3 years. Without a BIM, "economic benefit" is just a theory to a payer.
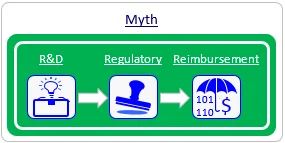
Myth #4: Reimbursement should be dealt with just prior to product launch.
Many of our clients initially see the commercialization process of their product as a serial process, starting with R&D, followed by regulatory related activities and, just prior to product launch, ending with reimbursement related activities. This serial process is depicted in the 'Myth' image on the right
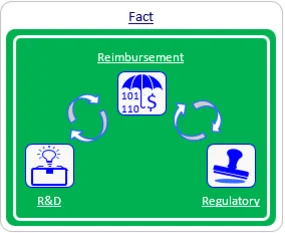
However, reimbursement activities may impact both R&D and regulatory aspects, as depicted in the 'Fact' image on the right and in the following real-life examples.
🛑 The Regulatory Success Trap
Many CEOs celebrate an FDA clearance only to realize they have no path to payment because their clinical trial endpoints didn't address payer requirements.
Don't let your clearance go to waste. Schedule a pre-clinical strategy review →
Real Life Examples
Impact on R&D activities
- Example #1: One of our clients developed a 4-sensor product that competed with other available 6-sensor products. This product was clinically superior and less expensive than its competitors. The company invited Mediclever to check whether it could utilize existing reimbursement mechanisms in France. A short assessment revealed available codes, a positive coverage policy, and payment rates that exceeded the company's expectations. However, the wording in the identified existing codes specifically indicated 6 sensors. Both possible alternatives - redesigning the product or developing new reimbursement mechanisms to suit the 4-sensor product - were too expensive at that stage. The company was left out of the French market.
- Example #2: A client in the field of chronic wound treatment developed and launched a product in the US market. Unfortunately, the pressure settings employed by its product deviated from the allowable range specified under existing reimbursement mechanisms. The CEO asked Mediclever to provide the company with a 'reimbursable' specification, and the company was compelled to redesign its product according to this specification.
Impact on regulatory activities
- Example #1: A company that had developed a diagnostic device asked Mediclever to start working on its reimbursement strategy after applying for, and receiving, regulatory clearance. Unfortunately, the wording that was used in the regulatory application substantially decreased the likelihood of reimbursement. On Mediclever's advice, the company re-applied for regulatory clearance with a modified indication for use. This delayed the launch of the product, resulting in substantial loss to the company.
- Example #2: One of our clients developed outstanding clinical data for its product and invited Mediclever to help it develop specific reimbursement mechanisms. Most of the payers that we approached were impressed by the developed clinical evidence, but wanted the company to also present data regarding some economic aspects. Because these economic aspects had not been observed during the company's previous clinical trial, the company had to perform a new trial to gather the requested data. Had the company thought about its reimbursement strategy prior to initiating the clinical trials, those economic aspects could have been integrated into its previous trials, making the investment in a new trial, and the delay in the sale of its product, unnecessary.
Summary
Frequently Asked Questions About Reimbursement Myths
Does a reimbursement code guarantee payment?
No. Reimbursement requires three pillars: a code, a coverage policy, and an established payment rate. A code without coverage results in no payment.
When should I start planning for medical device reimbursement?
Reimbursement strategy should be integrated early in the R&D and regulatory phases to avoid costly product redesigns or clinical trial gaps.
Are reimbursement criteria different in every country?
While procedural details vary, 99% of payers worldwide focus on two main criteria: significant clinical benefit over alternatives and economic benefit to the medical pathway.
Need Concrete Market Access Support?
Securing coverage and coding is the most critical step of your commercialization timeline. Our team maps global reimbursement pathways directly to your business goals.
About the Author
